
We appeal to the medical community and to the relevant national and international bodies to recognize the potential for airborne spread of coronavirus disease 2019 (COVID-19). There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several meters, or room scale), and we are advocating for the use of preventive measures to mitigate this route of airborne transmission.
Studies by the signatories and other scientists have demonstrated beyond any reasonable doubt that viruses are released during exhalation, talking, and coughing in microdroplets small enough to remain aloft in air and pose a risk of exposure at distances beyond 1–2 m from an infected individual ([1–4]). For example, at typical indoor air velocities [5], a 5-μm droplet will travel tens of meters, much greater than the scale of a typical room, while settling from a height of 1.5 m to the floor. Several retrospective studies conducted after the severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) epidemic demonstrated that airborne transmission was the most likely mechanism explaining the spatial pattern of infections [6]. Retrospective analysis has shown the same for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [7–10]. In particular, a study in their review of records from a Chinese restaurant observed no evidence of direct or indirect contact between the 3 parties [10]. In their review of video records from the restaurant, they observed no evidence of direct or indirect contact between the 3 parties. Many studies conducted on the spread of other viruses, including respiratory syncytial virus (RSV) [11], Middle East Respiratory Syndrome Coronavirus (MERS-CoV) [8], and influenza [2, 4], show that viable airborne viruses can be exhaled [2] and/or detected in the indoor environment of infected patients [11, 12]. This poses the risk that people sharing such environments can potentially inhale these viruses, resulting in infection and disease. There is every reason to expect that SARS-CoV-2 behaves similarly, and that transmission via airborne microdroplets [10, 13] is an important pathway. Viral RNA associated with droplets <5 μm has been detected in air [14], and the virus has been shown to maintain infectivity in droplets of this size [9]. Other viruses have been shown to survive equally well, if not better, in aerosols compared to droplets on a surface [15].
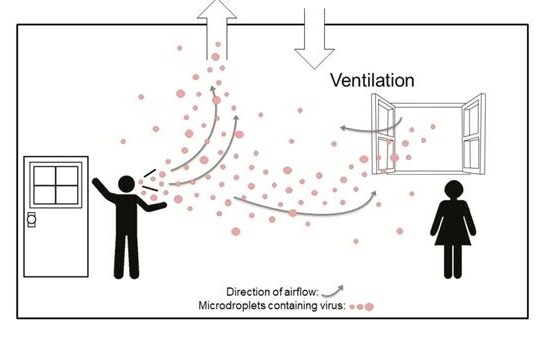
The current guidance from numerous international and national bodies focuses on hand washing, maintaining social distancing, and droplet precautions. Most public health organizations, including the World Health Organization (WHO) [16], do not recognize airborne transmission except for aerosol-generating procedures performed in healthcare settings. Hand washing and social distancing are appropriate but, in our view, insufficient to provide protection from virus-carrying respiratory microdroplets released into the air by infected people. This problem is especially acute in indoor or enclosed environments, particularly those that are crowded and have inadequate ventilation [17] relative to the number of occupants and extended exposure periods (as graphically depicted in Figure 1). For example, airborne transmission appears to be the only plausible explanation for several superspreading events investigated that occurred under such conditions [10], and others where recommended precautions related to direct droplet transmissions were followed. (…)